For confirmation and security purposes, all fields are required.
For help or questions, please call (000) 000-0000.
Our records indicate that you have not registered for myBlueCross yet. Please create an account to proceed.
How to find your group number
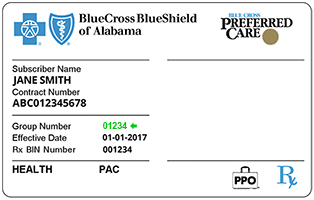
Your Group Number can be found on your Blue Cross and Blue Shield ID Card.
Blue Cross and Blue Shield of Alabama ID Card
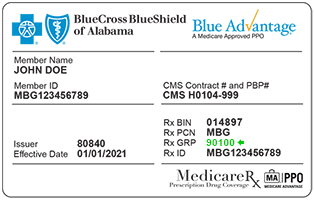
Medicare ID Card
No ID card yet? No problem.
Please contact Customer Service at 1-800-292-8868 for your group number.
Please Note:
FEP Members: If you are part of the Federal Employee Program (FEP), you should use Group Number 53533 when registering. If you wish to view claims or benefit information, please go to https://www.fepblue.org.
Postal Members: If you are part of the Postal Service Health Benefits (PSHB) Program, you should use Group Number 63715 when registering. If you wish to view claims or benefit information, please go to https://www.fepblue.org/our-plans/usps.
What is an ITIN?
An Individual Taxpayer Identification Number (ITIN) is a tax processing number issued by the Internal Revenue Service.
How to find your Medicare Number
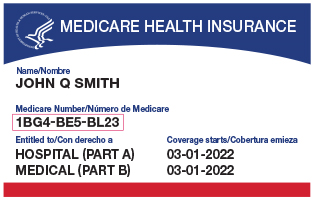
Your Medicare Number can be found on your red, white and blue Medicare Health Insurance card.
Medicare card image with Medicare Number identified
No Medicare card yet? No problem.
Please contact Social Security at 1-800-772-1213; TTY users can call 1-800-325-0778 for more information.